The audit everyone saw coming
HRSA’s 2026 wave of targeted audits didn’t catch anyone off guard. Covered entities running sprawling contract pharmacy networks were warned back in late 2025 that the Office of Pharmacy Affairs would begin enforcing strict data alignment between split-billing systems, contract pharmacy records, and EMR encounter files. The agency’s focus has clearly shifted, from basic eligibility checks to the deeper problem of data consistency: prescription origination, patient attribution, prescriber validation. In plain English, HRSA no longer cares just whether a refill qualifies; it wants proof that every system in your workflow tells the same story about that refill.
The first notices hit large delegated systems that expanded fast, building contract-pharmacy networks across multiple states. Hospitals pushing thousands of purportedly 340B-eligible prescriptions a month faced reconciliation gaps they couldn’t close. One Midwestern DSH hospital compliance officer told me HRSA flagged 300+ prescriptions where the prescriber NPI belonged to a site never registered as eligible, same patient, same day of service, but different origination truth in each data feed.
When split-billing systems drift apart
This audit cycle exposed a familiar weakness: split-billing discrepancy. Every seasoned 340B administrator knows the three-system tangle, EMR for encounters, split-billing for purchases, and a TPA platform handling contract pharmacy claims. Under HRSA’s 2026 audit protocols, those systems are now expected to behave like one record set. Any mismatch affecting a dispense’s 340B eligibility, wrong prescriber, wrong site, mismatched NDC, is a compliance risk, period.
It often begins innocently. A provider works a few days out of a satellite clinic, but the EMR still lists them under the hospital’s primary site. The split-billing engine processes it as parent-site eligible; the contract pharmacy processor labels it “satellite non-registered.” Multiply that error, and you’ve invited a six-figure repayment demand. Auditors don’t care that it was a “temporary setup.” They care that the data tell conflicting stories.
The systems keeping up now run nightly cross-checks, automated reconciliation scripts comparing split-billing logs to EMR prescriber tables. If you’re still doing quarterly spreadsheet audits, you’re already behind. When HRSA asks for “system integration validation,” they want timestamped verification that those automated controls actually run. Static documentation won’t save you anymore.
Prescription origination confusion in integrated networks
Another repeat offender this cycle: prescription origination errors. HRSA’s current take on “covered outpatient drug” within multi-site organizations hinges on where the prescription originated relative to registered child sites. Covered entities falter when a prescriber writes from an unregistered location even though the qualifying patient encounter occurred somewhere else. The mess ballooned after telehealth platforms began routing all prescriptions through central e-prescribe hubs.
At one FQHC I reviewed, telehealth visits were recorded under eligible sites, but the e-prescribing system defaulted to the administrative office’s NPI. HRSA threw out every claim, because the prescriber location metadata traced back to an ineligible site. The care was fine. The data made it noncompliant. Lesson learned: EHR configuration is now part of compliance. If your platform routes all scripts through a centralized NPI, you’re generating rejections by design.
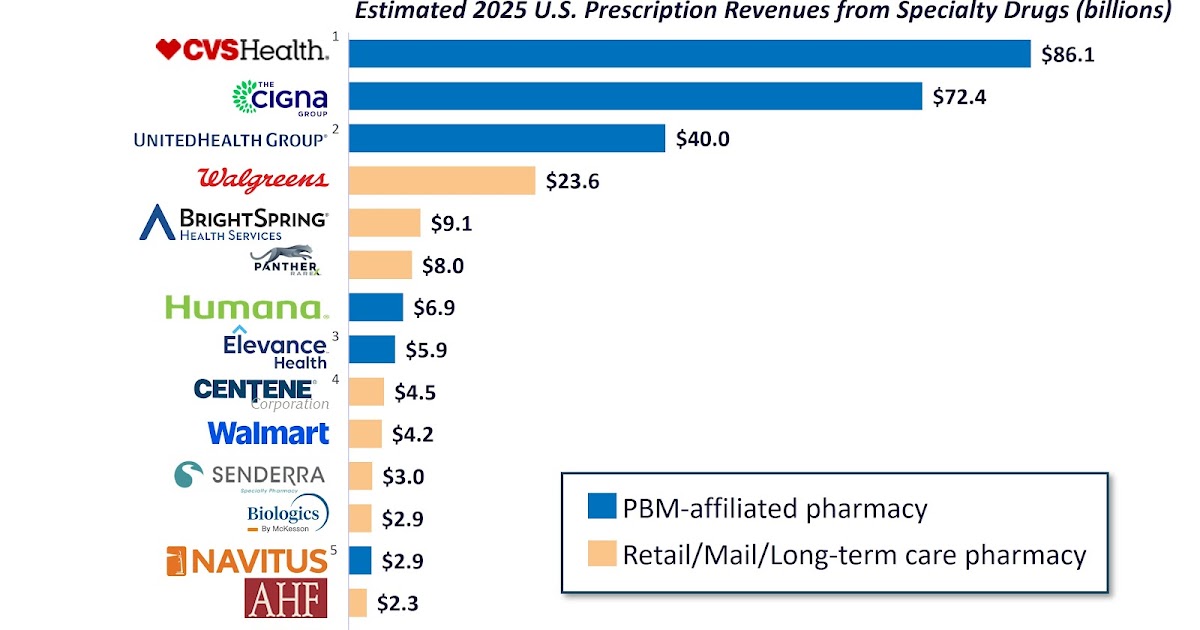
HRSA’s current FAQ set explicitly flags “prescriptions routed through consolidated prescriber IDs” for review. That’s a first. And it’s no coincidence that this aligns with what industry analysts like Adam Fein have been tracking about the 2026 PBM-health-system convergence. Those consolidated specialty and hospital-owned networks pool data across multiple 340B entities, exactly where HRSA is stress-testing data integrity. When PBM platforms control dispensing data and health systems hold encounter files, you’d better believe auditors will want proof the two align. Trust doesn’t factor in anymore.
How multi-site systems can stay defensible
Every compliance director knows HRSA won’t hand out a playbook. What it wants is proof of control, ongoing, automated, and backed by data. In 2026, that means your split-billing, EHR, and contract pharmacy feeds operate under the same logic. Most proactive systems now use middleware audit layers that validate NPI-site matches in real time before charge submission. Not fancy, just necessary. If you’re a hospital juggling dozens of prescribers and grant types, this integration is nonnegotiable.
Data provenance logging matters just as much. More entities are adopting immutable ledgers of prescription origination events, hashed timestamps, verifiable audit trails, so HRSA can retrace exactly which system marked a dispense as 340B-eligible. That replaces the vague attestations (remember the “TPA follows HRSA guidance” boilerplate?) that once passed for compliance. Now, the demand is proof: verifiable, reproducible, NDC-level proof.
And look, if senior leadership still treats 340B data validation as a paperwork chore, the next audit will change that attitude fast. The real compliance work in 2026 lives in the integration teams. It’s technical, relentless, detail-oriented. One stray prescriber-location mismatch today can cost more than adding a contract pharmacy did five years ago. The entities that embed data integrity into everyday operations, not just into their audit binders, are the ones sleeping better this year.


